Part D Policy Change Lowers Max OOP Costs for Many Enrollees
Summary
Cost-sharing reductions from enhanced plans and EGWPs allow beneficiaries to reach the catastrophic phase with lower OOP spending than those in basic plans.Background
The 2025 plan year has marked a turning point for Medicare Part D, with the redesigned benefit introducing a $2,000 out-of-pocket (OOP) cap and shifting how financial liability is shared across stakeholders.
As part of benefit redesign, the Centers for Medicare and Medicaid Services (CMS) also changed the definition of “incurred costs”—the expenses that count toward a beneficiary’s true out-of-pocket (TrOOP) costs and determine their progression through the Part D benefit. As of 2025, incurred costs now include supplemental spending on covered Part D drugs provided by enhanced alternative Part D plans, Employer Group Waiver Plans (EGWPs), and other health insurance. This means that any reduction in cost sharing provided by these plans below the defined standard benefit amount (25%) now counts toward TrOOP. Specifically, beneficiaries in enhanced plans or EGWPs advance through the benefit based on the greater of (1) their cost sharing under the defined standard benefit, or (2) the cost sharing under their plan design.
Most Part D plans use tiered formularies in the initial coverage phase rather than applying the 25% defined standard cost sharing to all drugs. Cost sharing on Tiers 1–3 is often lower than 25%, ranging from a copay of less than $2 on Tier 1 to about 20% coinsurance on Tier 3. While both basic and enhanced plans use tiered formulary structures, only cost-sharing reductions below the defined standard benefit count toward TrOOP for beneficiaries in enhanced plans or EGWPs. Because these cost-sharing reductions are now included in TrOOP, beneficiaries in enhanced plans or EGWPs can reach the OOP cap with considerably less than $2,000 in OOP spending.
Who has Reached the OOP Cap in 2025?
Avalere Health analyzed 2025 Part D Prescription Drug Event (PDE) data, accessed through CMS’s Chronic Condition Warehouse Virtual Research Data Center (VRDC), to examine how non-low-income subsidy (non-LIS) beneficiaries progressed through the redesigned benefit in the first two quarters of 2025.
Across all non-LIS beneficiaries who filled at least one Part D script through June 2025, about 8% reached the catastrophic phase. As EGWPs typically offer more generous benefits with lower cost sharing, a greater share of these enrollees (14%) reached the catastrophic phase in the first six months of the year compared to enrollees in enhanced and basic plans (7%). However, among those who reached the catastrophic phase, a greater share of basic plan enrollees did so in the first quarter of the year (41%) compared to beneficiaries in enhanced plans and EGWPs (32%).
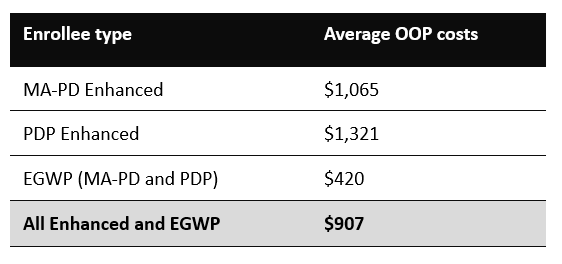
While non-LIS beneficiaries enrolled in basic plans generally reached the catastrophic phase with about $2,000 in OOP spending, beneficiaries in enhanced plans and EGWPs reached the catastrophic phase with lower OOP costs. EGWP enrollees had the lowest OOP costs to reach the catastrophic phase (less than $500 on average), while OOP costs were slightly higher for beneficiaries in enhanced PDPs compared to enhanced MA-PDs (Table 1).
Table 1. Average OOP costs among beneficiaries reaching catastrophic in the first 6 months (January – June) 2025
Considerations for Stakeholders
Manufacturers, plans, patient groups, and distributors should consider how lower OOP costs among beneficiaries in enhanced plans and EGWPs may impact utilization patterns, including adherence, initiation, and abandonment rates across therapeutic areas and drug types. Data from the first two quarters of the year also indicates that 9% of all non-LIS beneficiaries who reached catastrophic were enrolled in the Medicare Prescription Payment Plan (MPPP). Interactions between the OOP cap, counting of supplemental benefits toward TrOOP, and enrollment in the MPPP are also likely to affect beneficiary OOP costs and utilization differently across plan types.
As the Part D market continues to evolve, with more beneficiaries enrolling in Medicare Advantage and a reduction in standalone PDP options, stakeholders should consider how these dynamics combined with the Part D benefit changes may affect beneficiary OOP costs and utilization patterns. Emerging data on 2025 spending can also provide valuable insights to inform plan risk assessments, benefit design offerings, manufacturer contracting, and patient assistance program strategies in future years. Connect with us to learn more.
Methodology
This analysis utilized Part D PDE data through an agreement with CMS, wherein Avalere Health has access to CMS’s Chronic Condition Warehouse VRDC data. The analysis includes non-LIS Part D beneficiaries, with a script filled in the first six months (January through June) of 2025. Beneficiaries were assigned to enrollment in a specific plan type (basic, enhanced, or EGWP) based on the plurality of months they were enrolled in a plan in the first six months of the year. Beneficiaries were identified as enrolled in the MPPP if they had a script in the Part D PDE where MPPP enrollment was indicated. Avalere Health also analyzed beneficiaries who were either diagnosed with COVID-19 or filled a prescription for a COVID-19 medication, finding that just over 60,000 (or 2%) of non-LIS beneficiaries who reached catastrophic in the first two quarters of the year had COVID-19.
Services
produces measurable results. Let's work together.


