Part B Negotiated Drug Prices: How MA Plans Should Prepare
Summary
Part B drugs will be subject to IRA price negotiation for the first time in 2028, introducing new payment uncertainties for Medicare Advantage plans.On January 1, 2028, certain Part B drugs will be subject to negotiated maximum fair prices (MFPs) for the first time ever, per the Inflation Reduction Act (IRA). This is a significant inflection point: Part B drug negotiation introduces a new layer of operational and financial complexity, particularly for Medicare Advantage (MA) plans.
The drugs selected for Initial Price Applicability Year (IPAY) 2028 are currently prescribed to roughly 1.8 million Medicare beneficiaries and account for approximately $27 billion in combined Part B and Part D Medicare expenditures. Four of the 15 drugs (Botox, Cimzia, Entyvio, and Orencia) have a majority of their gross Medicare spending under the Part B benefit¹ and treat conditions ranging from autoimmune and inflammatory diseases to asthma and chronic urticaria.
Given differences in payment and coverage policies for Part B drugs between Medicare fee-for-service (FFS) and MA (Figure 1), understanding how MFPs will flow through the 2028 MA payment rates is now an urgent question for plans and providers.
Figure 1. Payment for Part B Drugs Differs between Medicare FFS and Medicare Advantage
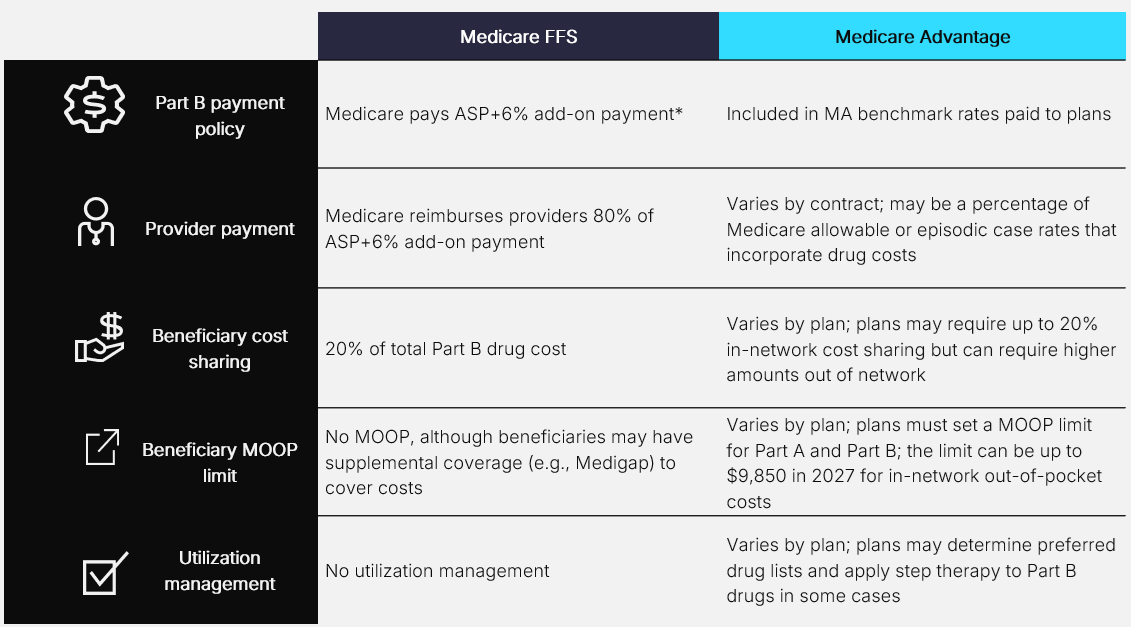
ASP: Average Sales Price; MOOP: Maximum Out-of-Pocket
*CMS has proposed to pay ASP – 33.4% for 340B acquired drugs in calendar year 2027
How the IRA Will Change Part B Drug Reimbursement
Beginning January 1, 2028, the four primarily Part B drugs, along with other negotiated products, will be reimbursed in Medicare FFS at 106% of MFP (minus sequestration), replacing the current ASP+6% methodology. This shift reduces provider payment for selected drugs to reflect the negotiated MFPs that will be lower than the current ASP. MFP price reductions for the IPAY 2028 drugs have not yet been announced and are expected later this year, meaning the full magnitude of the payment change remains unknown.
Because MA plans contract with providers using ASP-based reimbursement as a reference point, often paying a percentage of Medicare (e.g., 101% of Medicare), the shift from ASP to MFP will affect plan-provider contracting arrangements. Avalere Health has found that over 80% of commercial and MA contracts have at least a two-year duration, raising questions about whether and when those contracts will be renegotiated considering lower MFP-based benchmarks.
Key MA Implications: What Plans Should be Doing Now
As the MFP effectuation date approaches, there are several priority considerations that have potential financial implications for MA plans:
- Part B MFPs could lower MA benchmarks, with broad downstream impacts: CMS has not yet clarified how Part B MFPs will be incorporated in the MA benchmark rates that determine plan payments. MA benchmarks are derived from Medicare FFS per capita costs, meaning that as MFPs reduce FFS Part B drug expenditures, those savings could flow through to lower benchmarks in future rate-setting cycles, potentially impacting market stability, plan benefit design, utilization management (UM), and provider contracting. Plans should proactively model the potential benchmark impact of Part B MFPs and stress-test their benefit design and contracting assumptions accordingly.
- Part B MFPs may compound existing limitations in MA risk adjustment: Whether the Part B MFPs will be incorporated into risk adjustment in 2028 remains an open question that could further complicate MA plan payments. This uncertainty is compounded by the fact that the MA risk adjustment model has not been updated since 2024 and still relies on 2019 FFS expenditure data, meaning it may not accurately reflect current cost patterns. Even when the underlying data are eventually updated, the model will likely still not capture the true cost of Part B drugs, particularly newer, high-cost treatments where FFS expenditure data will always lag behind real-world utilization and pricing. As MFPs reduce expenditures for certain Part B drugs, the misalignment between benchmark policy and the risk adjustment model could introduce significant financial instability for MA plans. Plans should identify where negotiated drug savings are and are not reflected in their risk adjustment payments, and consider engaging with CMS to advocate for a methodology that more accurately captures the real-world cost of Part B drugs.
- Provider financial pressure may redirect Part B drug administration to higher-cost settings: Lower MFP-based reimbursement may put financial pressure on physician practices that acquire and administer Part B drugs. Avalere Health research on provider perspectives suggests that reduced margins could prompt shifts in site of care toward hospital outpatient departments, which are typically more expensive, potentially increasing total costs for MA plans even as unit drug prices fall. Plans should engage directly with physician practices administering high-volume Part B drugs to understand their financial pressures, while modeling the total cost impact of potential site-of-care shifts and incorporating those scenarios into network design and benefit planning.
- Part B MFP effectuation guidance could impact MA utilization management and benefit design: CMS is expected to release guidance on Part B MFP effectuation later this summer. This guidance could impact plan UM policies, including prior authorization, step therapy, and benefit design. Plans should begin reviewing their current Part B UM policies and benefit design frameworks now, so they are positioned to assess and respond quickly once CMS guidance is released.
The extension of IRA drug price negotiation to Part B drugs is not a distant policy question; MFPs will be announced later this year and take effect in 2028, well within current planning horizons for MA plan bids and provider contract cycles.
A Trusted Partner for MA Plans
Avalere Health’s drug pricing and coverage experts work closely with MA plans considering exactly how Part B drug negotiation will directly and indirectly impact benchmarks, risk adjustment, cost of care, utilization management, and benefit design. To learn more about how Part B drug negotiations may affect your organization, connect with us.
¹ Cosentyx and Xolair is also selected for IPAY 2028 negotiation and has both Part B and Part D utilization; however, its Part B utilization does not constitute a majority of spend for the product.
Services
produces measurable results. Let's work together.


