Exploring Disparities in Access Among Patients with Relapsed or Refractory Diffuse Large B Cell Lymphoma
Summary
Demographic and socioeconomic factors involved in treatment options in diffuse large B cell lymphoma oncology.Background
After decades of limited therapies for patients with relapsed or refractory diffuse large B cell lymphoma (R/R DLBCL), several innovative therapies have transformed the treatment paradigm. However, disparities can limit access to optimal care and worsen disease outcomes.
Avalere Health conducted a retrospective claims analysis to identify demographic and socioeconomic factors related to treatment options and potential barriers, starting at second-line therapy, where more innovative, complex, and expensive options are available.
Analysis
Avalere Health used Medicare fee-for-service (FFS) claims from 2018 through 2021 to identify patients with DLBCL and their associated therapies. Because there are no specific ICD-10-CM diagnosis codes for R/R DLBCL, initiation of second-line therapy was used as a proxy for progression to relapsed or refractory disease. Second-line therapy was defined as either the introduction of at least one new drug, biologic, or cell/gene therapy following first-line treatment, or a 180-day gap in therapy after first-line treatment.
Patients were assigned to one of five mutually exclusive second-line treatment cohorts:
- Chimeric Antigen Receptor T-cell therapy (CAR-T): CAR-T, regardless of other medications (highest priority cohort assignment); patients with any CART claims within 120 days of start of second-line of therapy
- Stem Cell Transplant (SCT):Allogeneic or autologous SCT, within 120 days after start of 2nd-line of therapy
- Innovative therapy (IT): Innovative therapies (e.g. biologics) during second-line of therapy
- Rituximab (Rtx)/Lenalidomide (LEN)-based Therapies (R/L): Includes Rtx alone, LEN alone, and Rtx combination with chemotherapy or LEN in second-line of therapy
- Chemotherapy (CT): CT alone.
Cohorts were described across a set of characteristics to elucidate any differences or notable findings.
Results
Between Jan 1, 2019 and March 31, 2021, 3,310 patients with R/R DLBCL were identified. Most patients were assigned to R/L cohort (61%), followed by CT alone and IT (14% each), and SCT and CART (5% each).
Table 1: Percentage of Second-line Therapy by Race/Ethnicity
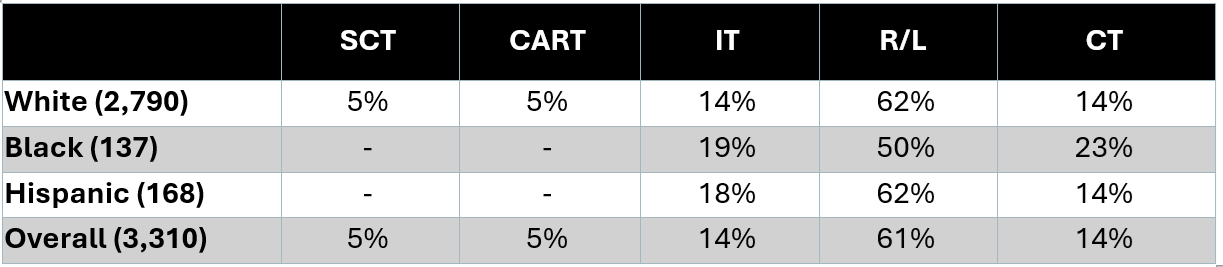
The majority of patients were White (84%), compared to only 4% Black/African American, and 5% Hispanic.
Compared to White and Hispanic patients, more Black/African American patients received CT and IT for second-line therapy and were more often treated in medical school-affiliated hospitals. Furthermore, Black/African American patients were younger at diagnosis compared to White and Hispanic patients. Black/African American patients in the CT cohort were from ZIP codes with lowest average household income ($55,762) across all racial/ethnic and Tx groups; overall, patients in the IT cohort were from ZIP codes with higher incomes compared to R/L across all racial/ethnic groups. Proportionally, use of CT and SCT therapies were slightly lower for Black/African American and Hispanic patients.
Conclusions
Chemotherapy and innovative therapies were more often administered to Black/African American patients with R/R DLBCL, than White or Hispanic patients. While seemingly incongruous, Black/African American patients more often received care for R/R DLBCL in medical school-affiliated hospital, which may be associated with more complex therapy options (CAR-T/SCT), but Black/African American and Hispanic patients both had lower utilization of these complex and expensive therapies. This analysis suggests economic factors and site of care both may impact accessibility of R/R DLBCL therapies, and sometimes conflicting ways.
Methodology
This analysis utilized the 100% Medicare FFS claims, accessed by Avalere Health via a research collaboration with Inovalon, Inc. and governed by a research-focused CMS Data Use Agreement.