White Paper: Estimated Federal Savings from the Special Diabetes Program
Summary
Avalere Health finds that research funded by the Special Diabetes Program has yielded more than $50 billion in federal healthcare savingsDiabetes affects more than 38 million people in the United States and remains the nation’s most costly chronic disease, with total costs reaching $413 billion in 2022. The Special Diabetes Program (SDP), created by Congress in 1997 and administered by the National Institutes of Health, provides federal funding to support research on the prevention, treatment, and potential cure of type 1 diabetes (T1D). While the program is focused on T1D, many of the innovations it has supported, such as continuous glucose monitors (CGMs) and automated insulin delivery (AID) systems, are now used more broadly, including among people with type 2 diabetes (T2D), and have contributed to improved outcomes across both populations.
To better understand the program’s economic impact, Avalere Health conducted an analysis of estimated federal cost savings associated with SDP-supported technologies. The analysis focused on direct medical expenditures and modeled the savings resulting from the use of CGM and AID systems by beneficiaries of public insurance including Medicare, Medicaid, and the Department of Veteran’s Affairs.
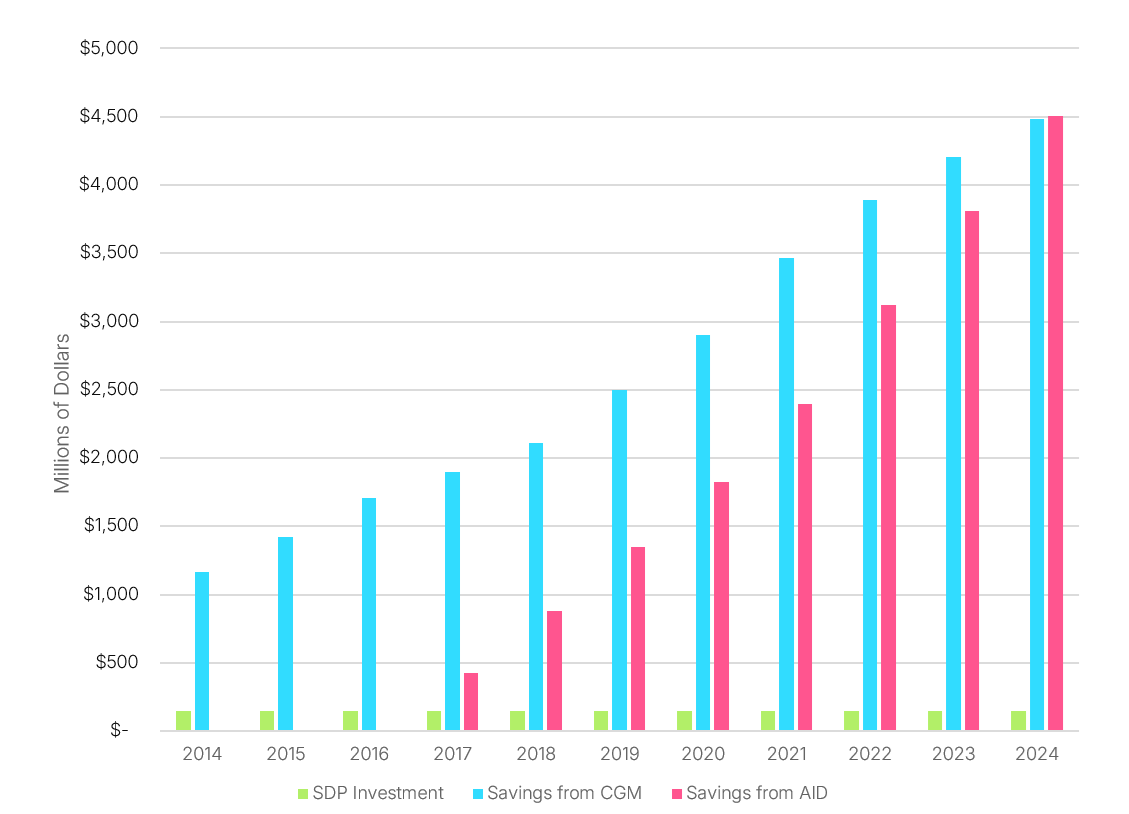
Findings indicate that CGMs and AID systems alone have generated at least $50 billion in federal healthcare savings through improved glucose management and reduced diabetes-related complications. Because the analysis does not include indirect cost savings such as improved productivity, reduced disability, or long-term prevention of complications, the actual federal savings and total economic impact of these technologies is likely higher.
Table 1. CGM and AID 2024 Utilization and Savings, Total Federal Savings from Start of SDP
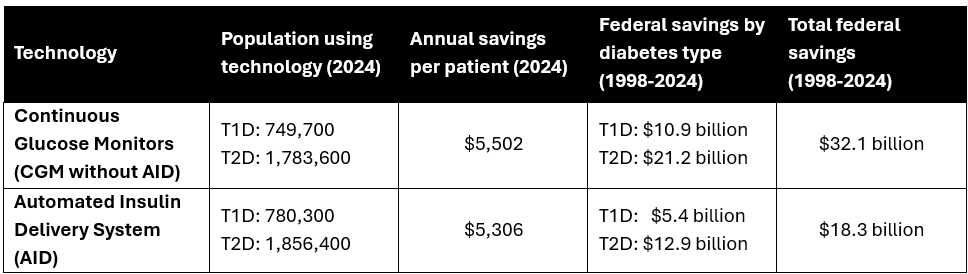
Each of the therapies examined in the model has benefited from SDP-supported research. For example, CGMs and AID systems were advanced through clinical trials and technology validation supported by the program. SDP-backed studies also contributed to the development of anti-vascular endothelial growth factor treatments for diabetic eye disease and to disease-modifying therapies such as teplizumab, which has been shown to delay the onset of clinical T1D. The program has also supported early-stage beta-cell replacement research, including the development of donislecel, the first Food and Drug Administration-approved allogeneic islet cell therapy.
Figure 1. Annual SDP investment and federal savings (2014-2024)
As policymakers evaluate the future of the SDP, stakeholders may consider how funding decisions will maintain or interrupt momentum in diabetes research and bringing advanced therapies to market. Disruptions in SDP funding may hinder clinical research infrastructure, delay scientific advancement, and slow patient access to therapies that reduce complications and lower overall costs. This study and existing literature confirm that the SDP has demonstrated a strong return on investment both clinically and economically. Ongoing support for diabetes research and treatments will be essential to realizing the full potential of emerging innovations for individuals with diabetes.
Funding for this research was provided by Breakthrough T1D (formerly JDRF). Avalere Health retained full editorial control.
Services
produces measurable results. Let's work together.


