Navigating State Variability in Medicaid Work Requirements
Summary
State discretion over work requirement implementation may create significant variability, impacting patients, providers, and health plans.On June 1, the Centers for Medicare & Medicaid Services (CMS) released an interim final rule with comment period (IFC) on Medicaid work requirements (what it calls “community engagement requirements”) to be implemented on January 1, 2027. Per the One Big Beautiful Bill Act (OBBBA), adults in states with Medicaid expansion or similar 1115 waivers must demonstrate 80 hours per month of qualifying “community engagement” activities to qualify for coverage.
The interim final rule establishes a federal framework for the requirements, but delegates key implementation decisions to states, creating conditions for significant variability in how the requirement is operationalized across the country. While the OBBBA requires states to implement work requirements by 2027, several states have announced earlier implementation dates, and Nebraska and Montana have already implemented their programs.
Where States Have Discretion
Medical Frailty Exemption
Certain individuals, including those who are “medically frail,” are exempt from the requirement. Per the OBBBA, the Secretary of Health and Human Services has discretion to define key terms related to the exempt population. The IFC describes a two-pronged approach to define individuals who have a serious or complex medical condition, prompting many stakeholders—including patient advocates and provider groups— to argue that CMS has gone beyond the statutory definition. To qualify for the exemption, an individual must both:
- Have a qualifying “serious or complex” medical condition, and
- Demonstrate that the condition significantly impairs their ability to comply with the work requirement.
While CMS provides definitions for these terms and sets the new standard for meeting medical frailty, it leaves many operational decisions to individual states:
- Qualifying Condition Lists: CMS requires states to develop their own lists of diagnoses, conditions, or diseases that may qualify for an exemption. Nebraska, prior to the IFC, published a 295-page index of over 6,800 diagnosis and procedure codes that could be considered for exemption. On the other hand, Montana took a higher-level approach, listing fewer than 100 diseases and conditions without specific codes. These methodological differences could result in significant discrepancies in beneficiary determinations across states.
- Verification Methodology: In the IFC, CMS provided limited guidance on how to measure functional impairment, leaving it to states to determine which data sources to use and how to weight clinical documentation against administrative data such as claims.
- Documentation Standards: States can set their own requirements for how to use claims or other data or what providers must submit to verify exemption status. This creates potential for inconsistent determinations based on how claims have been submitted or a provider’s capacity to document functional impairment.
Further, a lawsuit filed by 26 states argues that the serious and complex medical condition standard unlawfully narrows the statutory exemptions established by the OBBBA and unconstitutionally coerces states by imposing new compliance requirements after states have already invested in implementation based on prior CMS guidance.
The lawsuit requests a preliminary injunction that would place a six-month hold on work requirement implementation. If granted, this could potentially create further variability between states participating and not participating in the lawsuit.
Short-term Hardship Exemption
The OBBBA allows states to grant short-term hardship exemptions for individuals who face temporary barriers to compliance, such as hospitalization or a natural disaster. States may choose whether to offer this exemption, and if so, have discretion over qualifying events and duration. A state’s choice to offer the exemption means that a patient experiencing an acute exacerbation of a chronic condition may be protected from coverage loss in one state but not another.
These discretionary decisions will result in a patchwork of approaches across states, where a beneficiary with the same diagnosis and functional status could have two different determinations based on their state of residence.
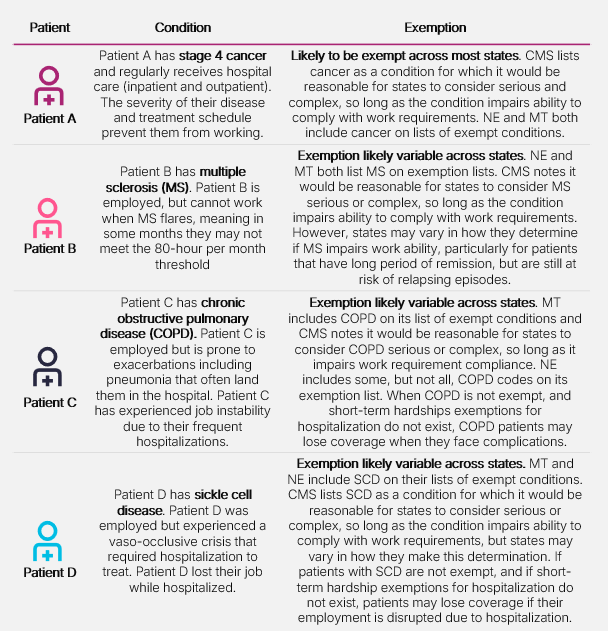
The following illustrative scenarios demonstrate how state decisions could produce meaningfully different outcomes for patients with similar health profiles.
Figure 1: Patient Scenarios: How the Same Condition Can Result in Different Outcomes Across States
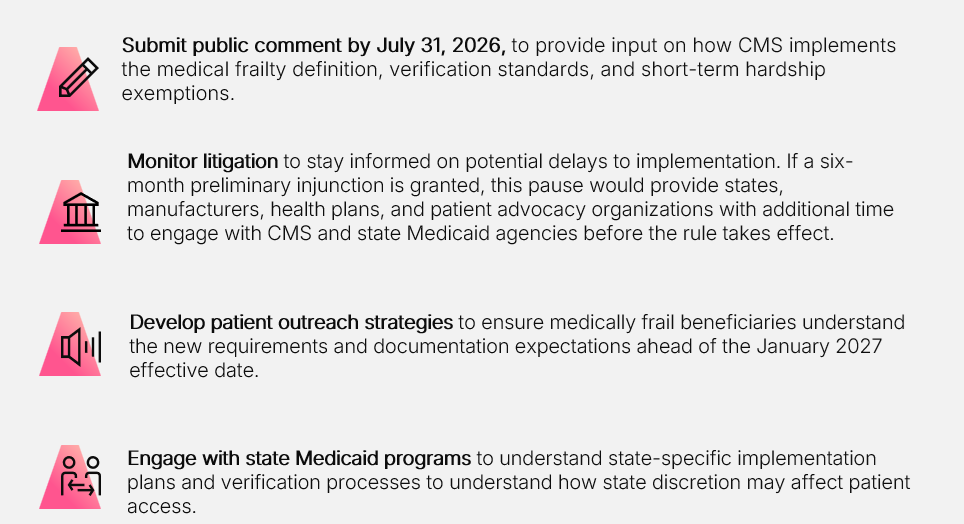
As work requirement implementation nears, stakeholders should:
Avalere Health is closely monitoring the implications of CMS’s work requirement for manufacturers, providers, and payers and the uncertainty they face as the details are refined. Our experts in Medicaid program requirements, state policy, patient access, and health data analytics help clients navigate Medicaid strategy and operations, patient access challenges, and health system patient mix. Connect with us to learn more about how Avalere Health’s team can help you prepare for the changes and shape the policy’s implementation in order to reach EVERY PATIENT POSSIBLE.
Read our other work requirement analyses:
- How Can Manufacturers, Payers, Providers, and Patient Groups Prepare for Medicaid Work Requirements?
- How can MCOs Prepare for Medicaid Community Engagement (Work) Requirements?
- Medicaid Work Requirements: Understanding Exemptions and Protecting Patients
Services
produces measurable results. Let's work together.