Multi-Stakeholder Collaboration in Rare Diseases: The Role of Clinicians Within and Beyond the Clinic
Summary
Clinicians can support timely, sustainable rare disease care through institutionalized multi-disciplinary roles, strengthened referral networks, and the translation of clinical insights into policy and advocacy.As part of a pro bono disease initiative exploring how multi-stakeholder collaboration can advance care for people living with rare diseases in Asia-Pacific (APAC), we are soliciting the views of patient groups, payers, clinicians and industry leaders. Complete this survey to share your perspective.
Introduction
In rare diseases, where knowledge is fragmented and evidence is scarce, clinicians are instrumental in providing critical context to guide multi-stakeholder discussions. They ensure that decisions are rooted in clinical realities and remain evidence-based.
Clinicians are not just care providers: They contribute to areas such as research, policymaking, and advocacy. In rare disease ecosystems, this expanded role is especially important, as limited evidence and concentrated expertise demand strong clinical leadership to generate knowledge, shape care pathways, and amplify patient needs within health systems.
In this fourth article of our Asia-Pacific rare disease series, we explore the levers for higher levels of multi-stakeholder collaboration from the clinician’s perspective, both within and beyond the clinical setting. Drawing on insights from Juliana Lee, certified genetic counsellor and Board of Directors Member of the Genetic Counselling Society Malaysia, we spotlight Malaysia as a case study to illustrate two dimensions of collaboration for clinicians.
- At the patient-care level, we explore how collaboration between clinicians can be strengthened to enable timely referrals and multi-disciplinary care for persons living with rare disease (PLWRD).
- At the health system level, we highlight how clinicians serve as catalysts for collaboration with other stakeholders through Malaysia’s National Rare Disease Committee.
Shortening the Rare Disease Diagnostic Odyssey
Timely and accurate diagnosis is the gateway to effective rare disease management. Yet for many PLWRD, their diagnostic journey takes an average of 7.6 years, eight physician consultations, and two to three misdiagnoses before the correct diagnosis is reached. The World Economic Forum describes this challenge as the “diagnostic dilemma,” driven by the unique and complex symptoms of rare diseases which challenge traditional models of care.
Unlike that of common diseases, rare disease management requires greater collaboration across health system tiers because specialized genetic expertise is often concentrated in few medical centers. For example, in Thailand, just 22 geneticists – predominantly located in major cities – serve a population of 67 million. Such workforce constraints underscore the need for coordinated referral pathways and system-wide collaboration to enable timely diagnosis and multi-disciplinary management across the patient journey.
In Malaysia, the absence of institutionalized genetic counselling services within the public healthcare system has resulted in PLWRD often being managed by physicians without formal genetics training, rather than being referred to qualified genetic counsellors or clinical geneticists. This gap in cross-disciplinary collaboration can delay diagnosis and compromise patient safety and quality of care. The lack of formally recognized roles for genetic counsellors has led to workforce attrition, with many locally trained professionals seeking employment overseas. This not only undermines the sustainability and quality of domestic rare disease care, but further constrains national capacity. Recognizing this, Malaysia’s 2025 National Policy for Rare Diseases emphasizes the need for timelier referral of PLWRD and their families to genetic counselling. The policy also calls for dedicated budget allocations to enhance genetic counselling services within the public sector, while fostering collaboration with private genetic counselors and laboratory services.
This dynamic in Malaysia highlights a broader challenge in rare disease management across APAC. Health systems must proactively identify gaps in essential roles and service offerings, ranging from genetic specialists, allied health professionals and social workers, and institutionalize them by clearly defining their scope of practice, establishing structured training programs, and embedding them into care pathways.
However, ensuring the supply and availability of multi-disciplinary care is only half the equation. Health systems must also enable access by strengthening collaboration across clinical networks that connect hospitals of different tiers of care. Below, we highlight China as a case study to illustrate the impact of the National Network to Collaborate on Diagnosis and Treatment of Rare Diseases and the Peking Union Medical College Hospital (PUMCH) model.
Figure 1: China’s National Network to Collaborate on Diagnosis and Treatment of Rare Disease and PUMCH Model
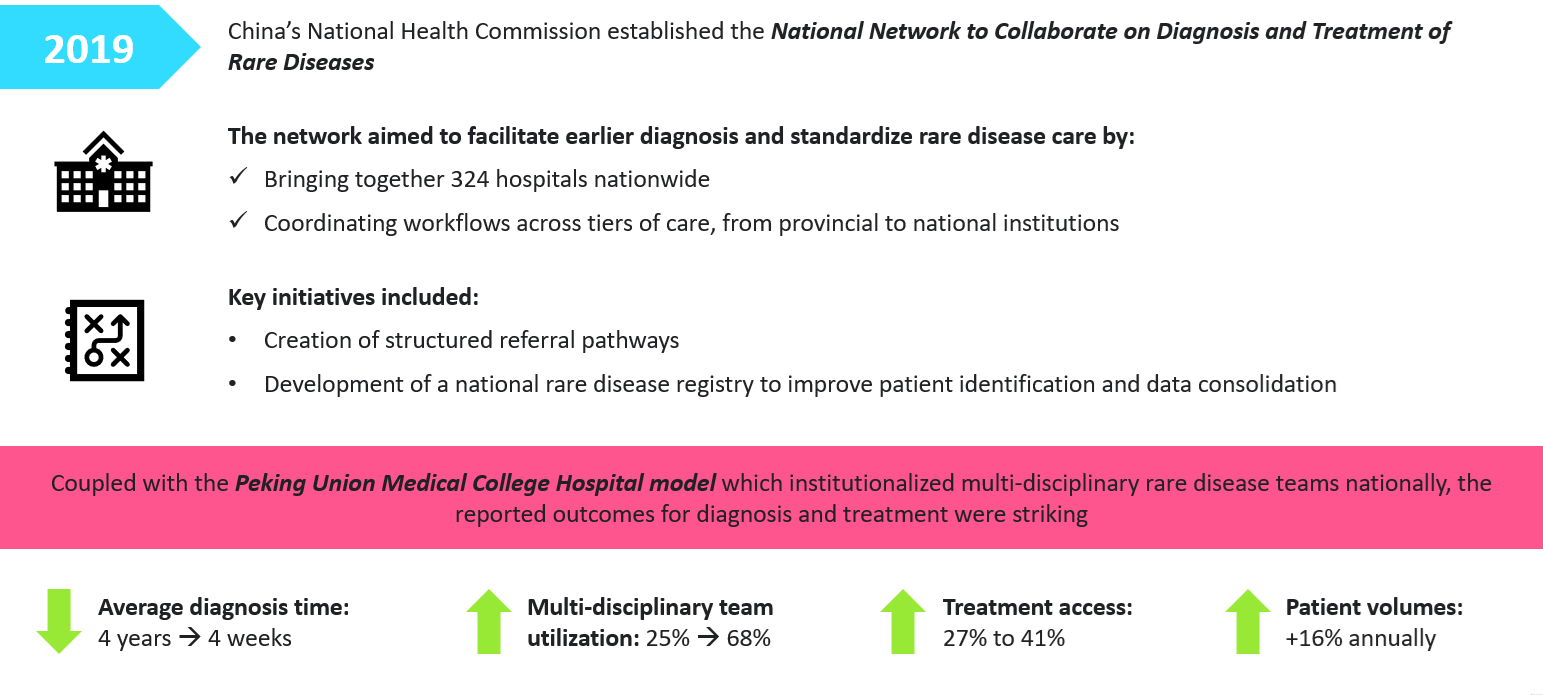
Strengthening rare disease care requires both institutionalized clinical roles to ensure the availability of specialized expertise, and system-wide collaboration to enable timely access to that expertise. Embedding structured multi-disciplinary collaboration within care networks can transform fragmented pathways into more equitable, efficient, and sustainable rare disease care in APAC.
Bridge Clinical Knowledge Gaps
Beyond collaboration within clinical settings, clinicians play a pivotal role in bringing medical experience and insights into discussions with non-clinical stakeholders. Their ability to interpret complex clinical evidence and contextualize it within health system realities enables more informed decision making among policymakers, payers, and patient groups. In the context of policy decisions, clinicians help bridge clinical experience and legislative frameworks, ensuring that healthcare policies are evidence-based and patient-centered.
In 2019, the Ministry of Health Malaysia established the National Rare Disease Committee as a multi-stakeholder platform, bringing together specialist geneticists, genetic counsellors, patient groups, and Ministry of Health representatives. The Committee, chaired by the Deputy Director General of Health (Medical), convened regularly and operated through dedicated technical working groups covering clinical management, orphan drug access, advocacy and health education, and health technology assessment, ensuring holistic and coordinated input across the rare disease pathway.
In an interview, genetic counselor Juliana Lee shared that the Committee was the product of years of sustained joint advocacy by clinicians, alongside patient groups and other stakeholders to elevate rare diseases as a policy priority. Rare diseases, given their low prevalence, often receive limited attention within healthcare systems. Clinicians are uniquely positioned to elevate rare diseases as a priority by synthesizing fragmented patient experiences into clinically meaningful evidence that informs system-level decision making.
Within multi-stakeholder collaborations such as Malaysia’s National Rare Disease Committee, clinicians contribute by virtue of their expertise, relationships and influence. For example:
- Clinician involvement ensures that policy directions are grounded in real-world care delivery, helping shape strategies that are both relevant and feasible.
- Clinicians’ professional standing and networks across clinical communities allow them to represent the interests of frontline providers while also translating complex medical knowledge into terms that non-clinical stakeholders can act upon.
- Clinicians’ formal authority and informal influence enable them to build consensus and mediate discussions among diverse stakeholders, fostering shared vision and sustained collaboration.
This demonstrates how clinicians, especially those who also serve in ministry or advisory roles, can serve as catalysts in shaping policies that are anchored in clinical realities and patient-centered priorities. Malaysia’s National Rare Disease Committee exemplifies this, where sustained multi-stakeholder collaboration translated cross-sector perspectives into actionable policy and ultimately supported the launch and implementation of the National Policy for Rare Diseases.
Conclusion
In APAC rare disease care, clinicians are central to enabling effective multi-stakeholder collaboration. Within clinical settings, institutionalized roles ensure the availability of multi-disciplinary expertise, while structured referral pathways enable timely, coordinated care across disciplines. Beyond the clinic, clinicians translate medical knowledge into actionable insights for policymakers, payers, and patient groups, helping align diverse stakeholders around shared priorities. By bridging clinical practice and system-level decision making, clinicians serve as the keystone of coordinated, patient-centered care and sustainable health system improvements.
Play a role in the APAC rare disease space? Share your perspectives via a short survey to share your perspective
Note: All comments and opinions expressed by the interviewees in this article are their own and do not necessarily reflect the views or positions of their respective organizations.
~
This is the fourth installment of our APAC rare disease series, exploring how multi-stakeholder collaboration can advance care for PLWRD. Explore our other articles below:
Services
produces measurable results. Let's work together.


