Are Cost-Effectiveness Thresholds Fit for US Reimbursement Decision-Making? Methodological, Practical, and Policy Considerations
Summary
Cost effectiveness thresholds present conceptual and practical challenges when applied to the US healthcare system.Cost-effectiveness (CE) methods have long been debated by health economists and healthcare decision-makers across systems around the world. In the context of the US healthcare system, however, the role of CE thresholds (CETs) as reimbursement ceilings has received limited evaluation. Avalere Health recently undertook an evidence-based analysis of the conceptual and practical challenges associated with standardized CE thresholds, considering their relevance and suitability in the United States’ healthcare system.
Methods
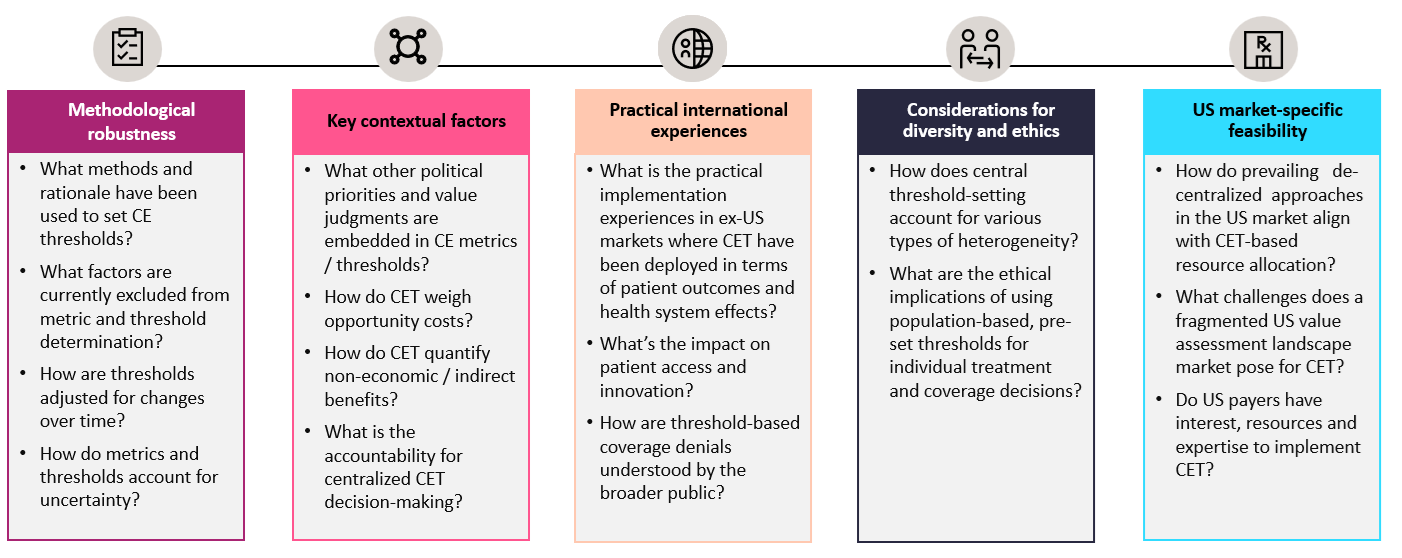
A qualitative research approach was used to assess the broader discourse on the use of CE thresholds in healthcare decision-making. We conducted a targeted literature review across five domains: implementation experience, contextual and institutional factors, technical robustness, US-specific implications, and social/ethical considerations. The full list of included sources are provided in the Appendix.
Figure 1. Domains for key research questions on the CE analysis (CEA) threshold evidence landscape
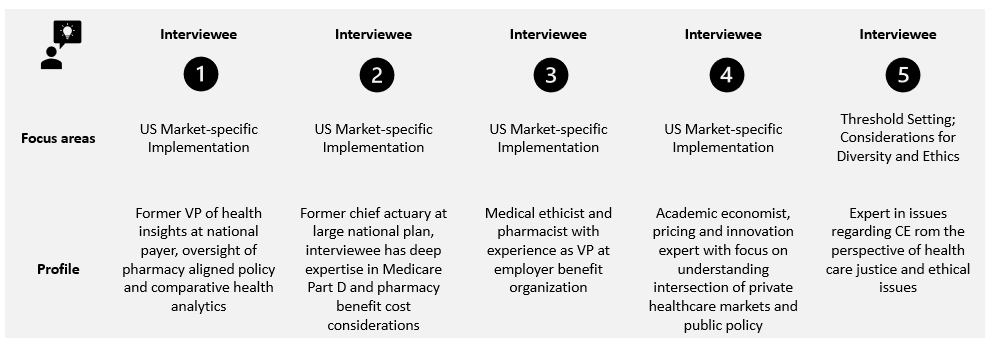
Subsequently, we conducted two rounds of semi‑structured interviews with ten experts (five based in the United States and five based outside the United States), including economists, payers, ethicists, and former health technology assessment decision-makers to explore international use cases and US transferability. Interviews were double blinded: Interviewees were not informed of the study sponsor, and the sponsor was not provided the identities of individual interviewees. Participants were chosen by Avalere Health to reflect diverse institutional perspectives and practical experience with CE methods. Notes and transcripts were anonymized and coded, and findings were thematically synthesized across the five analytic domains. Our analysis of the literature and interviews with experts illustrates the key issues with thresholds and is not intended to be exhaustive.
The first five interviews focused on the international application of thresholds, conceptual parameters, and ethical considerations. The second round of interviews focused on relevance and transferability of concepts for US payer decision-making and ethical considerations in the US context.
Figure 2. Overview of Round 1 Interviewees: International Focus

Figure 3. Overview of Round 2 Interviewees: US Transferability Focus
Research Synthesis
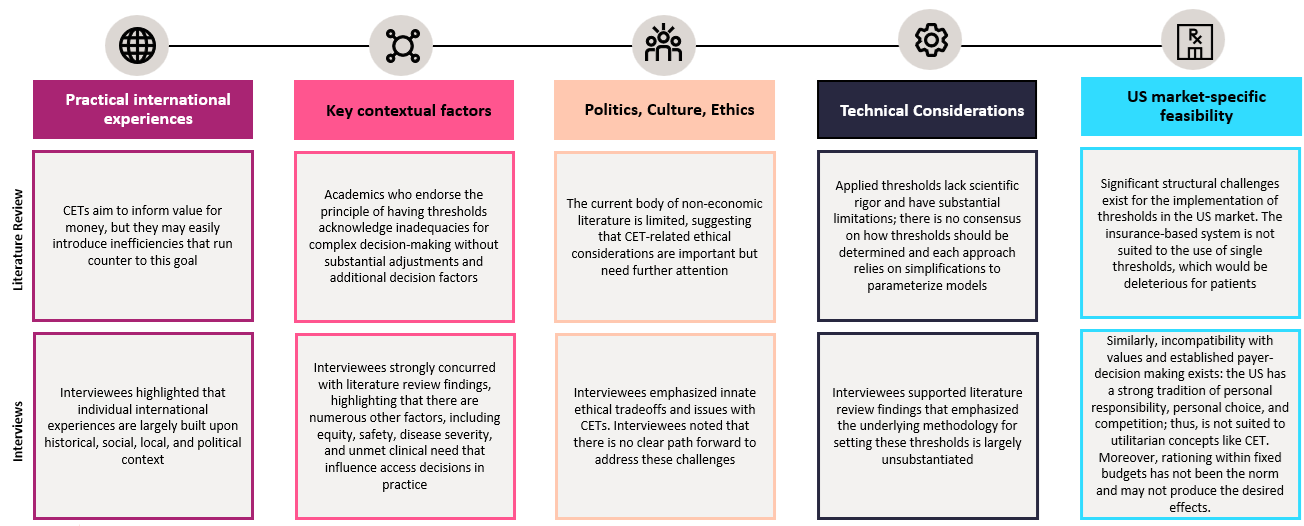
We found that articles in the pharmacoeconomic literature examine varied approaches to CE threshold setting and that each methodology has implicit tradeoffs. Further, research found that implementation of each methodology may lead to different thresholds, with potential access implications. Interviews indicated that practical experience with international applications revealed substantial variation in how CE thresholds are used: some countries have rejected them, while others apply them inconsistently, rely on bypass mechanisms, or introduce contextual adjustments to moderate their effects in practice.
Supporters of CE methods have claimed that even imperfect frameworks can offer a transparent starting point for evaluating trade-offs. Our analysis examined whether threshold-based approaches are suited to the institutional realities and decision-making demands of the American healthcare market. The US market is decentralized and multi-payer, with hundreds of health plans serving distinct groups of beneficiaries, and payers often competing on benefit design, access, and responsiveness to patient and employer priorities. In the US, heterogeneous patient needs, diversity in payer management objectives and populations, and the importance of individual choice all complicate the feasibility of leveraging CE approaches that are conceptually rooted in societal preferences for a given country.
Our research identified a fundamental disconnect between threshold-driven CE approaches and the realities of the decentralized US healthcare system. US decision-makers emphasized the importance of flexible, context-sensitive approaches to value assessment that preserve local agency and account for patient characteristics and payer objectives. The assumptions that often underlie CE threshold frameworks, including uniform valuation of health gains, fixed budgets, and centralized health priorities, do not align with the distributed nature of US healthcare, where priorities, resource constraints, and decision contexts vary across plans and populations. Stakeholders pointed to the advantages of the current US system (i.e., decentralized flexible decision-making), including its ability to accommodate diverse priorities, support patient-centered care, and foster a range of financing and insurance arrangements tailored to different beneficiary populations.
Taken together, our findings suggest that the scientific base of CE thresholds is grounded in several variable methodologies, their ex-US implementation has been more complex in practice, and their underlying premises are not aligned with the structure and values of the US healthcare system.
As such, significant challenges exist in implementing CE frameworks with fixed thresholds for access and reimbursement decision-making in the US.
Figure 4: Domains to assess evidence on setting CETs
Key Learnings
Our analysis highlighted several challenges and risks associated with relying on CE thresholds as a key determinant of whether an intervention should be covered and funded in any healthcare system, particularly in the US. The research explored these issues in greater detail through literature and expert interviews and highlighted the following key themes, summarized below.
Methodological reflections:
- There is no single methodological “gold standard” for threshold setting or use. No widely accepted scientific rationale has resolved how thresholds should be derived, calibrated, or operationalized, and real-world administration varies substantially across and within countries.
- Threshold-based frameworks are designed to optimize population-level economic efficiency under narrow assumptions. In doing so, they rely on standardized utility metrics and simplified decision rules that may conflict with individualized care, patient-centered value, and broader ethical principles of justice.
- A single evaluative standard may disadvantage some therapies for reasons unrelated to their underlying value. Standardized approaches to evidence assessment can penalize therapeutic areas where measurement is more difficult or where study design is constrained by the nature of the condition, such as small populations, heterogeneous disease presentation, or ethical limits on randomization.
- CE analyses are point-in-time forecast models. Their results depend on the data, comparators, and researchers’ assumptions selected when the analysis is conducted. As evidence, prices, and treatment pathways evolve over a product’s lifecycle, a therapy may move above or below a threshold even when the same methodology is applied.
Learnings on ex-US CE thresholds:
- Budgets are rarely fixed in practice. Resource decisions in practice are made within budgets that can and need to be flexible for adaptation relative to broader environmental, political, and cultural considerations.
- Systems that use CE thresholds introduce exceptions or modifiers. Severity adjustments, rare disease modifiers, budget impact overrides, and other contextual mechanisms have emerged in practice because unbending single-threshold approaches did not accommodate real-world population needs.
- Explicit thresholds may distort market dynamics. By signaling payers’ willingness to pay, they can weaken incentives for value-based competition, alter pricing behavior, and distort incentives for future medical investment and innovation.
- Thresholds used in centralized systems prioritize maximum population benefit over personalized care and individual patient choices
- Threshold-based CEA processes may add procedural requirements that delay or complicate access. When CE analysis becomes a formal gating mechanism, additional review, negotiation, managed-access arrangements, or reassessment can postpone patient access and deter launch or uptake of new treatments.
- Contextual factors around population-wide threshold approaches contrast with US market realities where plans serve diverse and often highly specific beneficiary populations, and they tailor coverage decisions to their own populations, priorities, and budget realities rather than to a single decision rule or uniform coverage authority.
Literature and Interviews Elucidated Significant Complexities in Use of CETs
In summary, our review of literature and expert interviews suggests that the use of CE thresholds for drug coverage decisions faces considerable challenges in the United States. Issues reflect broader debates over the role of CE analysis in access and reimbursement, but they also extend beyond familiar concerns associated with controversial metrics such as the quality-adjusted life years (QALYs). As we learned throughout this project, CE thresholds are not neutral technical parameters. Rather, they are policy constructs that depend on methodological choices, normative judgments, and assumptions about budgets, comparability, and decision authority. Taken together, the academic literature, real‑world experience outside the US, and stakeholder perspectives suggest that CE theory rests on several assumptions that often do not hold in practice.
In practice, international experience is varied and muddled. Multiple frameworks coexist across non‑US systems; few jurisdictions that incorporate CE analysis rely on a single threshold in a rigid or mechanistic manner; and where thresholds are used, they require exceptions, modifiers, negotiations, or other adaptations to account for clinical complexity and societal priorities. Whether such approaches yield value determinations that are more efficient, transparent, accountable, or equitable than those used in the United States remains unclear.
The US healthcare system is decentralized, the populations it serves are heterogeneous, and multi‑payer decision‑making is organized around the needs and priorities of specific beneficiary groups rather than a single national decision rule. Health plans assess value from different perspectives, within distinct budgetary and contractual realities, and for the beneficiaries they directly manage. At the same time, cultural and societal preferences place a high value on individual choice, clinical discretion, competition, and continued medical innovation. While imperfect, existing and emerging US approaches to value assessment allow decision‑makers to weigh these considerations in more tailored and context‑sensitive ways.
Implication for US Policy-Makers
Across both the literature and expert interviews, we found potential barriers regarding the use of predetermined CE thresholds for value-for-money resource allocation in the US, reflecting unresolved conceptual challenges, tension with US values, as well as potential for unintended consequences for market competition and dynamic efficiency.
In the United States, concerns about CE frameworks do not stop with the use of QALYs. The QALY has been subject to explicit legal and political rejection over the years, as federal law such as the Inflation Reduction Act bars the use of QALY-based measures for coverage, reimbursement, or incentive decisions in Medicare Drug Price Negotiations. This reflects long-standing societal discomfort with reliance on summary measures in ways that could devalue the lives of elderly, disabled, or terminally ill patients.
Our analysis, however, showed that the threshold against which such measures are applied also raises a separate and equally important set of questions. A CE threshold as a de facto reimbursement ceiling is not a neutral technical benchmark; it is a policy construct that depends on specific normative judgments and institutional assumptions about budgets, priorities, comparability, and decision authority.
The barriers and challenges that exist within ex-US markets are likely to be exacerbated in the US market, where there is a heterogeneous population, there are strong cultural and societal preferences for individual choice and innovative options in health care, and decision-makers have varying flexibility in their health care budgets. Decision-makers are decentralized and assess value from their own and the population they manage perspectives, rather than the societal perspective, enabling coverage decisions that can be more specifically tailored to generate value for a more localized population.
The use of CE thresholds requires underlying assumptions that are often fraught with inconsistencies, as documented in academic literature and our stakeholder interviews. In addition, experts describe various unresolved practical tensions in systems around the world, and the unique underlying framework of the US healthcare system elucidates several incompatibilities with the implementation of cost-effectiveness thresholds in the US. These dynamics are a key consideration for policymakers who seek to promote value-based care and efficient healthcare spending.
This Insight was funded by Johnson & Johnson. Avalere Health retained full editorial control.
References
References reviewed as part of the targeted literature review are as follows:
Betram, M. Y., Lauer, J. A., Joncheere, K. D., Edejer, T., Hutubessy, R., Kieny, M-P., Hill, S. R. Cost-effectiveness thresholds: Pros and cons. Bull World Health Organ. 2016; 94(12):925-930.
Beresniak, A., A. Medina-Lara, J. P. Auray, A. De Wever, J. C. Praet, R. Tarricone, A. Torbica, D. Dupont, M. Lamure, and G. Duru. 2015. “Validation of the underlying assumptions of the quality-adjusted life-years outcome: results from the ECHOUTCOME European project.” Pharmacoeconomics 33 (1): 61-9. https://doi.org/10.1007/s40273-014-0216-0.
Brekke KR, Dalen DM, Straume OR. The price of cost-effectiveness thresholds under therapeutic competition in pharmaceutical markets. J Health Econ. 2023;90:102778.
Browne, John, Donna R. Cryer, and William Stevens. 2021. “Is the QALY Fit for Purpose?” American Journal of Managed Care, July 14. https://www.ajmc.com/view/is-the-qaly-fit-for-purpose-.
Cairns, J. Using cost-effectiveness evidence to inform decisions as to which health services to provide. 2015;2(1), 32–38.
Camejo, R. R., Miraldo, M., Rutten, F. Cost-effectiveness and dynamic efficiency: Does the solution lie within? Value Health. 2017:20(2):240-243.
Cameron D., Ubels J., Norström, F. On what basis are medical cost-effectiveness thresholds set? Clashing opinions and an absence of data: a systematic review. Glob Health Action. 2018;11(1):1447828
Canadian Agency for Drugs and Technologies in Health (CADTH). Guidelines for the Economic Evaluation of Health Technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017.
Cleemput, I., Neyt, M., Thiry, N., De Laet, C., Leys, M. Using threshold values for cost per quality-adjusted life-year gained in healthcare decisions. International Journal of Technology Assessment in Health Care. 2011;27(1):71-76.
Cubi-Molla, P., Errea, M., Zhang, K., Garau, M. Are cost-effectiveness thresholds fit for purpose for real-world decision making? OHE Consulting Report. Office of Health Economics. Available at: Are Cost-Effectiveness Thresholds fit for Purpose for Real-World Decision Making? – OHE
Dubois RW. Cost-effectiveness thresholds in the USA: are they coming? Are they already here? J Comp Eff Res. 2016;5(1):9-11.
Gafni, A., and S. Birch. 1995. “Preferences for outcomes in economic evaluation: an economic approach to addressing economic problems.” Soc Sci Med 40 (6): 767-76. https://doi.org/10.1016/0277-9536(94)e0109-6.
Garrison, L. P., Jackson, T., Paul, D., Kenston, M. Value-based pricing for emerging gene therapies: The economic case for a higher cost-effectiveness threshold. 2019; 25(7):793-799.
ICER. Frequently Asked Questions. 2025. https://icer.org/who-we-are/faqs/
FDA. Framework for FDA’s real-world evidence program. 2018. Available here.
Luyten J, Denier Y. Explicit cost-effectiveness thresholds in health care: a kaleidoscope. Soc Justice Res. 2019;32:155-171.
Marseille, E., Kahn, J. G. Utilitarianism and the ethical foundations of cost-effectiveness analysis in resource allocation for global health. Philosophy, Ethics, and Humanities in Medicine. 2019(5).
Moradpour J, Hollis A. The economic theory of cost-effectiveness thresholds in health: domestic and international implications. Health Econ. 2021;30(5):1139-1151.
National Council on Disability. 2019. Quality-Adjusted Life Years and the Devaluation of Life with a Disability. November 6. https://www.ncd.gov/report/quality-adjusted-life-years-and-the-devaluation-of-life-with-a-disability/.
Neumann, P. J., and J. T. Cohen. 2018. “QALYs in 2018-Advantages and Concerns.” Jama 319 (24): 2473-2474. https://doi.org/10.1001/jama.2018.6072.
Neumann, P. American exceptionalism and American health care: Implications for the US debate on cost-effectiveness analysis. OHE Briefing, No. 47. 2009. Available here.
Neumann PJ, Sanders GD, Russell LB, Siegel JE, & Ganiats TG. (2017). Cost-Effectiveness in Health and Medicine (2nd ed.). New York, NY: Oxford University Press, p. 4.
Refoios Camejo, R., Miraldo, M., Rutten, F. Cost-effectiveness and dynamic efficiency: Does the solution lie within? Value Health. 2017: 20(2):240-243.
National Institute for Health and Care Excellence (NICE). Guide to the Methods of Technology Appraisal 2013. London: NICE; 2013.
Pearson, S. D. The ICER value framework: Integrating cost effectiveness and affordability in the assessment of health care value. Value Health. 2018: 21(3):258-265.
Sampson, C., Zamora, B., Watson, S., Cairns, J., Chalkidou, K., Cubi-Molla, P., Devlin, N., Garcia-Lorenzo, B., Huges, D., Leech, A. A., Towse, A. Supply-side cost-effectiveness thresholds: Questions for evidence-based policy. Appl Health Econ Policy. 2022;20(5):651-667
Schlander, M. 2010. “Measures of efficiency in healthcare: QALMs about QALYs?” Z Evid Fortbild Qual Gesundhwes 104 (3): 214-26. https://doi.org/10.1016/j.zefq.2010.03.012.
Schwarzer, R., Rochau, U., Saverno, K., Jahn, B., Bornschein, B., Muehlberger, Flatscher-Thoeni, M., et. al. Systematic overview of cost-effectiveness thresholds in ten countries across four continents. J Comp Eff Res. 2015;4(5)485-504.
Seixas, B. V., Dionne, F., Conte, T., Mitton, C. Assessing value in healthcare: Using an interpretive classification system to understand existing practices based on systematic review. BMC Health Services. 2019;19:560.
Sorenson, C., Lavezzari, G., Daniel, G., Burkholder, R., Boutin, M., Pezalla, E., Sanders, G., McClellan, M. Value Health. 2017; 20(2):299-307.
Grutters, Janneke P.C., Anouck Kluytmans, Gert Jan van der Wilt, and Marcia Tummers. 2022. “Methods for Early Assessment of the Societal Value of Health Technologies: A Scoping Review and Proposal for Classification.” Value in Health 25 (8): 1227–1234. https://doi.org/10.1016/j.jval.2022.03.004.
Pharmaceutical Research and Manufacturers of America (PhRMA). 2023. Global Access to New Medicines Report. April. https://cdn.aglty.io/phrma/global/resources/import/pdfs/2023-04-20%20PhRMA%20Global%20Access%20to%20New%20Medicines%20Report%20FINAL-1.pdf.
Vallejo-Torres, L., Garcia-Lorenzo, B., Castilla, I., Valcarcel-Nazco, C., Garcia-Perez, L., Linertova, R., Polentinos-Castro, E., Serrano-Aguilar, P. On the estimation of cost-effectiveness threshold: Why, what, how? Value in Health. 2016: 558-556.