Physician Payment Changes and MFP May Strain Independent Physicians
Summary
Medicare payment and Part B drug pricing changes may increase financial pressure on certain independent physician practices, varying by specialty and site of care.Medicare Physician Payment
Medicare reimburses physicians under the Medicare Physician Fee Schedule (MPFS), which is updated annually. Payment for each service is determined by the relative value unit (RVU) assigned to that service, multiplied by the conversion factor (set annually), and adjusted for geography, quality, and sequestration. The higher a service’s RVU, the higher the physician payment. Thus, changes in RVUs affect physician reimbursement, with the magnitude of impact driven by both the size of the RVU change and service volume.
The total RVU for a service reflects the sum of three components:
- Work RVU: Accounts for the clinician’s time, effort, skill, and intensity required to furnish a service
- Practice expense (PE) RVU: Captures the cost of operating a practice, including both direct costs (e.g., clinical labor, supplies, equipment) and indirect costs (e.g., administrative overhead)
- Professional liability RVU: Reflects malpractice insurance costs
While the work and professional liability RVUs do not vary by site of care, the PE RVU differs depending on where a service is delivered. In the CY 2026 MPFS Final Rule, the Centers for Medicare and Medicaid Services (CMS) updated the methodology for allocating indirect PE to services furnished in facility settings: It set the indirect PE per work RVU at 50% of the amount used for non-facility services, resulting in lower total PE RVUs for facility-based services.
RVU and Physician Impact Analysis
To assess the impact of PE RVU changes on physician payment, Avalere Health analyzed 100% Medicare fee-for-service (FFS) Part B Carrier claims from CY 2025 and identified all services billed by physician practices in select specialties. Total RVUs were calculated by applying both CY 2025 and CY 2026 RVUs to CY 2025 service volume for each practice. To isolate the impact of RVU changes on payment, the CY 2025 conversion factor was applied to both years to estimate and compare total reimbursement.
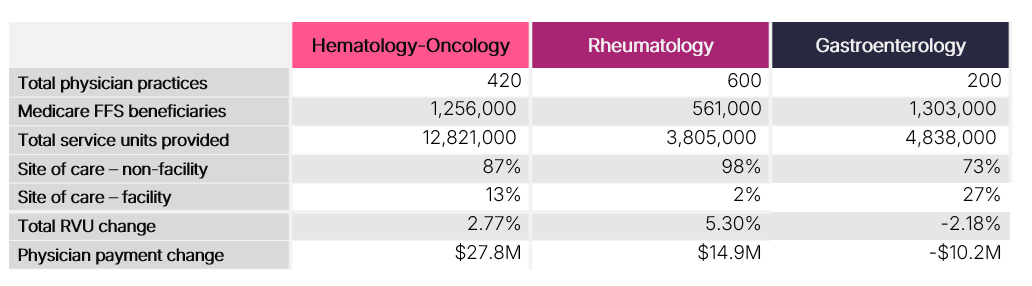
The analysis focused on three specialties: hematology-oncology (hem-onc), gastroenterology (GI), and rheumatology. Holding the conversion factor constant, specialties with a higher proportion of services delivered in non-facility settings (hem-onc and rheumatology) may experience increases in payment due to higher PE RVUs in these settings in CY 2026. In contrast, specialties with a greater share of services delivered in facility settings, such as GI, may experience decreases in estimated payment. These changes are primarily driven by PE RVU adjustments, as work and professional liability RVUs were, on average, similar between CY 2025 and CY 2026.
Table 1 summarizes changes in RVUs and associated payment impacts from CY 2025 to CY 2026. When isolating RVU-driven changes and holding the conversion factor constant, estimated payments increase by approximately $28 million for hem-onc and $15 million for rheumatology, while GI is projected to experience a decrease of approximately $10 million in CY 2026.
Table 1. Table 1. Change in RVUs and Physician Payment from CY 2025 to CY 2026
Medicare Part B Price Negotiation
Under the Inflation Reduction Act’s (IRA’s) Medicare Drug Price Negotiation Program, CMS will establish a maximum fair price (MFP) for a select number of drugs each year. Beginning in Initial Price Applicability Year 2028, Part B drugs will be eligible for selection. Prior Avalere Health research examined the potential implications of this policy on physician reimbursement.
Currently, most Part B drugs are reimbursed based on the product’s average sales price (ASP), plus a 6% add-on payment. This percentage-based add-on, which is subject to sequestration, is intended to support provider acquisition and handling costs, including storage, inventory management, and other operational requirements associated with physician-administered therapies. Under the IRA, reimbursement for negotiated drugs will be based on the MFP, which is expected to be lower than ASP. As a result, total reimbursement for these drugs will decline, which will increase financial pressure on physician practices.
MFP and Physician Impact Analysis
Because policy and payment changes may interact and compound over time, Avalere Health assessed the combined impact of changes in physician payment (described above) and the potential effects of Part B drug price negotiation. The timing of these policies is not aligned, as the physician payment analysis compares CY 2025 to CY 2026, while Part B drug price negotiation will not begin until 2028. Accordingly, this analysis is intended to illustrate the directional and additive effects of these policies rather than provide a precise estimate of future payment changes.
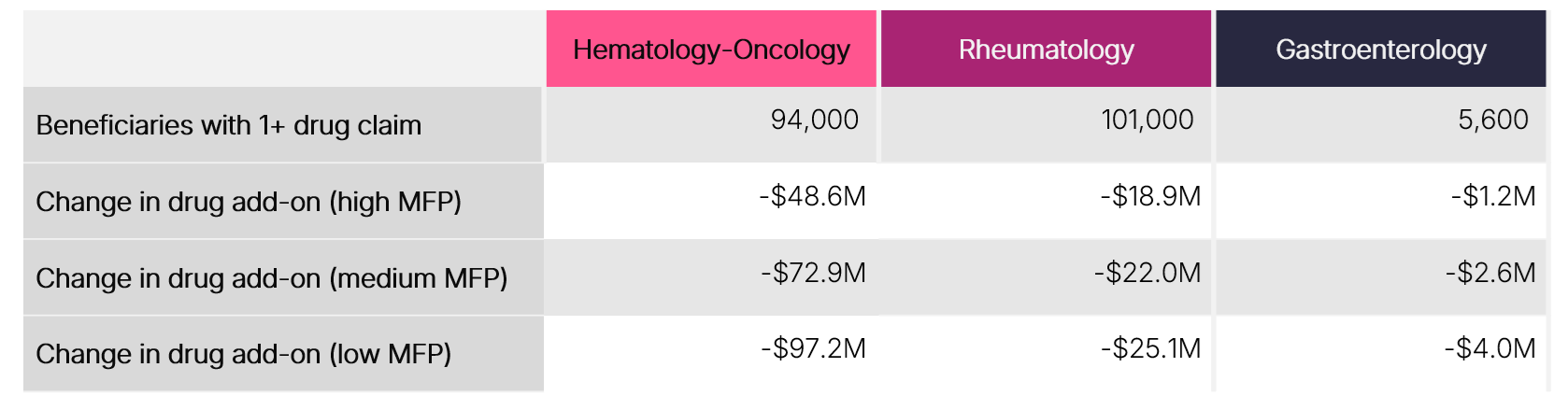
Avalere Health analyzed 100% Medicare FFS Part B Carrier claims from CY 2025 to quantify utilization and associated add-on payments for 11 drugs that may be eligible for Part B price negotiation between 2028 and 2032. This analysis assesses the magnitude of add-on payments tied to these products within a single year and models the total add-on amounts that could be affected under different negotiated pricing outcomes. Scenario analyses were conducted using three potential MFP levels—high, medium, and low—to reflect a range of possible reductions from current ASP-based reimbursement.
As noted above, the add-on payment associated with Part B drug reimbursement supports the overhead needed to acquire, store, administer, and manage these therapies. While reimbursement may shift from ASP- to MFP-based payment, these underlying costs are not expected to change. As negotiated prices decrease relative to ASP, the add-on payment would also decline, reducing the support available for these practice expenses.
Dollars at risk for add-on payments are greatest for hematology-oncology practices, ranging from $49–$97 million, followed by rheumatology ($19–$25 million) and gastroenterology ($1–$4 million) (Table 2). These findings reflect both utilization patterns and reliance on these payments to sustain care delivery infrastructure.
Table 2. Change in Physician Add-on Payment when Transitioning from ASP to MFP
 Combined Impact
Combined Impact
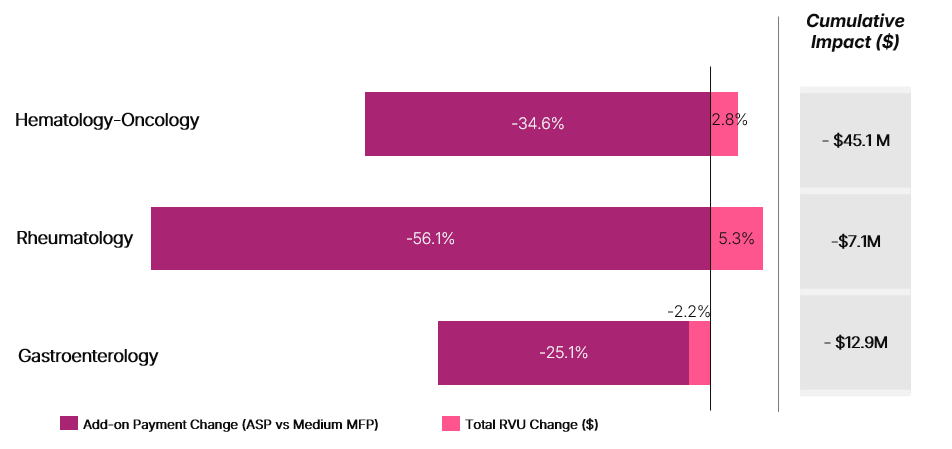
As noted above, physician payment changes effective in CY 2026 will precede the implementation of MFP for Part B drugs, and not all drugs included in this analysis would be subject to negotiation in the same year. Accordingly, this scenario is intended to illustrate the additive effects of these policies rather than reflect a precise estimate of future payment changes. Assuming a medium MFP scenario, Figure 1 presents the combined change in physician payment and reductions in Part B drug add-on payments.
The aggregate impact of these payment changes will vary by specialty, based on differences in service mix, site of care, and Part B drug utilization. For hem-onc and rheumatology, the physician payment provides a near-term payment increase, but represents only a fraction of the Part B add-on payment at risk for products that may be negotiated.
Figure 1. Payment Change Resulting from Changes to RVU (2025 to 2026) and Medium MFP Add-on Payment (6% of ASP to 6% of Medium MFP)
Stakeholder Implications
Changes to physician payment and Part B drug pricing may create cumulative pressure on physician practices in coming years, particularly those with a higher share of services delivered in facility-based settings and significant Part B drug utilization. Even where physician payment for services provided are neutral or favorable, such as in hem-onc and rheumatology, there will still be reductions in drug add-on payments under MFP.
As CMS advances payment reform, policymakers may consider how these changes interact and whether certain specialties or sites of care are disproportionately affected. Potential unintended consequences include practice or site closures, reduced patient access to care, and shifts in care delivery to higher cost settings (e.g., hospital-based settings), which may increase certain costs for patients and payers.
Stakeholders may assess site-of-care exposure, evaluate reliance on Part B drugs that may be subject to MFP, and model the combined effects of RVU and MFP changes across service lines. In addition, stakeholders may consider how operational and care delivery strategies could adapt to a reimbursement environment that is increasingly constrained and sensitive to policy pressures.
Connect with us to learn more about how Avalere Health supports client’s policy, access, pricing, contracting and channel strategy related to Part B negotiations.
Methods
Avalere Health analyzed 100% Medicare FFS Part B Carrier claims from CY 2025 through an agreement with CMS, wherein Avalere Health has access to CMS’s Chronic Condition Warehouse Virtual Research Data Center. The analysis included 11 drugs likely to be selected for Medicare Part B price negotiation. Avalere Health identified physician practices that administered any of the 11 drugs and assigned practices to a specialty based on taxonomy. For each practice, Avalere Health assessed all physician service utilization in CY 2025. Using the service mix from CY 2025, Avalere Health leveraged CY 2025 and CY 2026 MPFS rate tables and the CY 2025 conversion factor; this approach isolated the impact of RVU change on physician payment. MFP values were estimated using the latest guidance available from CMS at the time of analysis.
Services
produces measurable results. Let's work together.


